Anemia is a condition where a patient’s red cells are fewer than normal, usually reflected by low hemoglobin.
Anemia of chronic kidney disease is very common in CKD patients, especially in the later stages.
Tangled in the knotty problems of blood pressure and blood sugar, electrolytes and water balance, CKD patients and their treating teams often overlook anemia of chronic kidney disease.
Nevertheless, anemia is easy to diagnose and treat, offering an opportunity to keep kidney disease patients healthy and symptom-free.
What Causes Anemia in CKD
Low Erythropoietin
Our bone marrow is a factory for forming different blood cells—one of them is red cells. This cell-forming gel fills the bones of our back, chest, and pelvis, as well ribs. However, the bone marrow needs several supporting substances to produce red cells. One of them is erythropoietin.
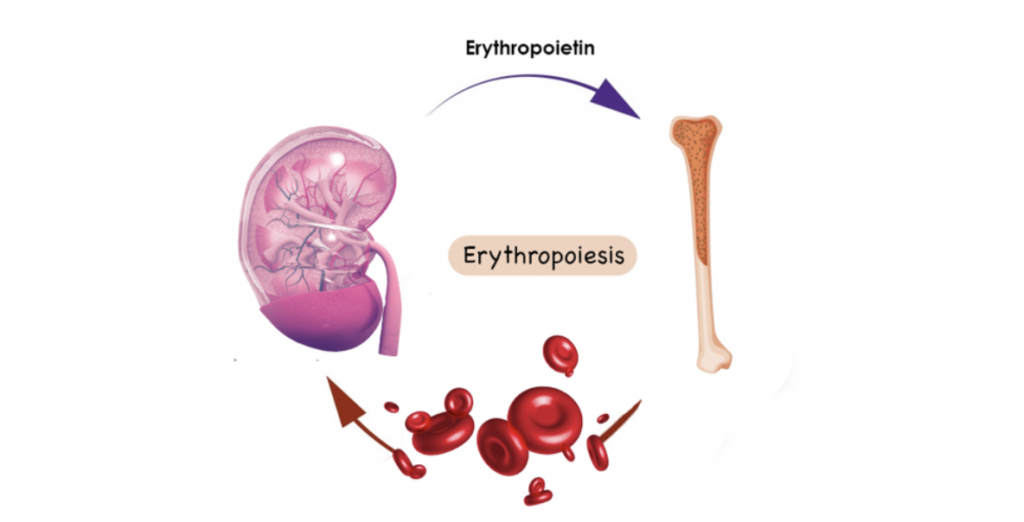
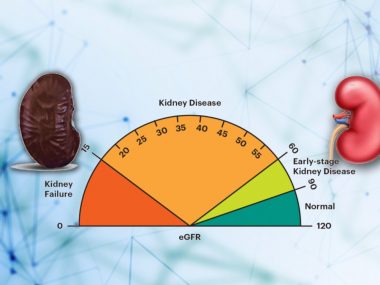
Erythropoietin is a hormone secreted by the kidney, and its level in the body is directly related to kidney health. As kidneys grow weaker, starting at eGFR 60 but more notably below eGFR 30 ml/min, erythropoietin level drops, resulting in CKD-related anemia.
Low Iron Level
Another common reason for anemia of chronic kidney disease is inadequate iron, an essential ingredient for red cell production. In a CKD patient, the supply of iron to the bone marrow is interrupted by many factors. Common factors are blood loss from the intestinal tract, chronic infections, and poor folic acid and vitamin B12 absorption. Most importantly, however, kidney disease blocks the release of iron from storage cells. It is like you have money in your bank, but you cannot withdraw it, while you are starving to sickness.
Vitamin B 12 and Folic Acid deficiency
A deficiency of these vitamins can occur in some CKD patients, especially in the late stages, when a restricted diet and diminished digestion inevitably lead to malnutrition.
Diagnosing Anemia—Simple but Tricky
For diagnosing anemia, you need a blood test called complete blood count or CBC. A hemoglobin level of 13 or below for males older than fifteen means anemia. For females older than age fifteen, hemoglobin below 12 confirms the diagnosis.
Anemia of chronic kidney disease is slightly different in the sense that more than one condition might contribute to the low cell count and, accordingly, require a detailed workup.
This workup involves four blood tests related to the level of iron in the body—total iron level, an iron-binding protein, ferritin, and transferrin saturation. Using these values, your doctor figures out all the causes of anemia. More often, kidney disease patients have a combination of anemia from chronic kidney disease and anemia from iron and erythropoietin deficiency.
Learning about iron deficiency is crucial because if a patient has iron deficiency as well, we need to find its cause and fill the tank with iron before giving erythropoietin.
Symptoms of Anemia
- Weakness
- Fatigue
- Shortness of breath with minimal activity
- Problem with concentration
- Headache
- Dizziness
- Swelling in ankles
- Paler
How Do You Treat Anemia
Iron Supplements
Treatment of anemia of chronic kidney disease starts with boosting iron levels. For this purpose, iron pills work well in the early stages of kidney disease. But in the later stages, iron from the pills fails to absorb, necessitating iron infusions, meaning injecting iron through blood vessels.
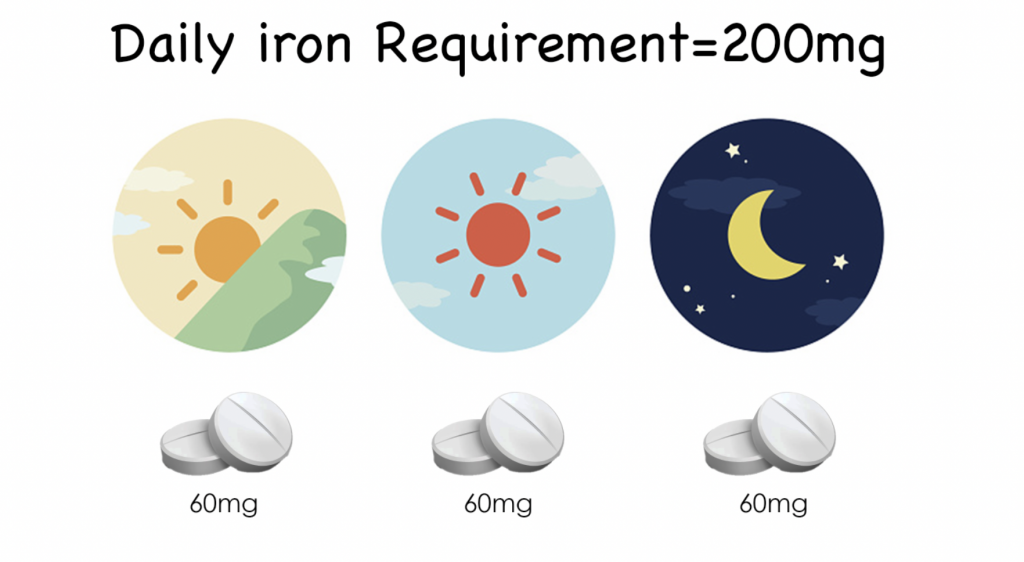
The treatment requires taking at least 200 mg of elemental iron daily. One tablet contains around 60 mg of iron. Thus, you need three pills a day to meet the target dose of 200 mg. However, there are some formulations that patients take once a day.
Iron pills are notorious for upsetting the GI tract, common symptoms being heartburn and constipation. You can address these symptoms by taking iron pills with food. However, you should avoid taking iron tablets with antiacid medications and dairy products, both of which decrease iron absorption from the gut.
Rarely, iron pills prove so intolerable for some patients that they need to switch to iron infusions.
Once your iron stores are replete, kidney disease patients need another tonic for using this iron to form red cells.
Erythropoietin
Erythropoietin is now commercially available in the synthetic form. It is injected under the skin a few times weekly, depending on the patient’s need.
It is recommended when hemoglobin drops to 9 or below, with the target of achieving a hemoglobin level of 11.5. This recommendation is based on research; when the researchers tried to achieve higher levels of hemoglobin, above 11.5, in CKD patients, a significant portion of the study population got a heart attack or stroke. Some patients’ blood pressure started to shoot, too.
Additionally, erythropoietin has been shown to increase tumor growth and is usually avoided in patients with actively treated cancer.
At any rate, erythropoietin is not suitable for every CKD patient. Its role comes only in the late stages of kidney disease, particularly after starting dialysis.
Before We are Done
In a kidney disease patient, anemia is common in the late stages. With this lower level of hemoglobin, the capacity of blood to transport oxygen decreases, leading to the symptoms of anemia. If you are a kidney disease patient, ask your doctor to check for anemia, particularly iron levels, for hemoglobin levels drop after the iron has been low for an extended period.
Moreover, folic acid and vitamin B 12 levels, though not a typical feature of kidney disease, can be low in CKD patients, partly due to absorption issues and partly due to poor appetite and the resulting malnutrition. Some nephrologists regularly check and replace them.
Further Reading
https://consultqd.clevelandclinic.org/anemia-of-chronic-kidney-disease/