Reducing proteinuria forms the cornerstone of chronic kidney disease management. The last decade has seen the addition of many protein-reducing medicines, each with its unique set of traits. Along comes the Finerenone, a protein-reducing medicine with an even more brilliant set of features.
Finerenone is now an FDA-approved drug for proteinuria treatment in diabetic kidney disease alone. However, this kidney-protective drug can potentially treat chronic kidney disease of any origin, a point still awaiting validation with research. Furthermore, although it attracted attention for its protein-reducing capacity in diabetic patients, ignoring other inherent properties of this medicine that can doubly benefit kidney disease patients would be unfair.
To grasp all the benefits of Finerenone, one must first understand the management of chronic kidney disease.
Components of chronic kidney disease management
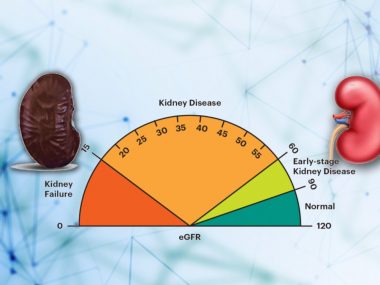
Chronic kidney disease is not a specific condition in itself; it is rather a common pathway, the final pathological state of the kidney, regardless of the method of damage. The kidney damage of any origin, lasting long enough to trigger chronic inflammation and fibrosis in the kidneys, leads to chronic kidney disease. The diagnosis of chronic kidney disease requires a higher-than-normal level of creatinine for at least three months.
Once your doctor confirms that you have chronic kidney disease, he manages it with three strategies deployed simultaneously.
Treatment of the underlying cause
First is the treatment of the condition that damaged the kidney in the first place. For example, if you have hypertension or diabetes, you need to control your high blood pressure and sugar. Similarly, an autoimmune kidney disease, such as IgA nephropathy and membranous nephropathy, calls for medicines to suppress your immune system.
Treatment of kidney disease complications
Second, treatment of kidney disease complications. Chronic kidney disease patients develop many complications. Water and salt retention leads to swelling in the body, requiring diuretics. High blood pressure, both a cause and a complication of kidney disease, needs lifestyle changes and blood pressure medicines. Autoimmune kidney diseases call for immunosuppressives. As a part of this strategy, Finerenone rises above other drugs, as we will see in a moment.
Treatment of proteinuria
The third and most important of all strategies is to control of leakage of protein in the urine. Reducing proteinuria, along with lifestyle changes and other kidney disease management components, requires specific medicines. And to this list of these medicines, Finerenone is the latest addition.
How does Finerenone reduce urine protein?
Imagine a room full of ammunition, but the door is locked. Opening the door requires the key, which can unleash many bad things. If you want to keep that door shut so that bad things don’t happen, there are many ways to do so, but one simple trick can be the use of a mock key that is very similar in shape to the original key and even fits in the lock, yet it prevents the door from opening, and at the same time precludes the insertion of the original key. Now, let’s name the original key aldosterone and the ripoff, Finerenone.
Finereone, a synthetic molecule, mimics a natural hormone in our body called aldosterone. Both of them have an affinity for a specific receptor called mineralocorticoid receptor. Biologically, aldosterone and related hormones bind to mineralocorticoid receptors expressed in many tissues, such as the heart and kidney, and many cells, such as immune cells. This interaction is essential for keeping the body’s fluid and electrolytes in balance and blood pressure in range. However, the overactivation of this system—more aldosterone production, which then binds to more receptors—has many unwanted consequences: excess retention of fluid and salts, higher blood pressure, and, finally, inflammation and fibrosis of the heart and kidneys.
When Finerenone docks at the mineralocorticoid receptor, it prevents the attachment of aldosterone to these receptors, blocking the downstream harmful effects of the hyperactive aldosterone system. In short, the door remains locked, and bad things, checked.
Why is Finerenone good for kidney disease?
Scientists have reasons to believe that this mineralocorticoid hyperactivity forms an important aspect of chronic kidney disease development and progression. And traditional kidney disease medicines, angiotensin-converting-enzyme inhibitors and angiotensin-receptor-blockers, have a limited role in suppressing this system, clearly showing a need for a new drug with the capability of directly blocking this axis, which is where the Finerenone comes in.
Benefits of Finerenone—Protienuria reduction
Finerenone slows down the progression of kidney disease and reduces the leakage of proteins in the urine. Moreover, it reduces the risk of heart-related complications in kidney disease patients.
Although it benefits both diabetic and non-diabetic kidney disease patients, rigorous research supporting its use is only available for the former.
Diabetic kidney disease
Currently, only two significant trials have studied the effects of this drug, and both enrolled only diabetic kidney disease patients. Based on the data from one of these trials, FIDELIO-DKD, the FDA approved the use of this medicine for diabetic kidney disease patients for the following purpose: “reduce the risk of kidney function decline, kidney failure, cardiovascular death, non-fatal heart attacks, and hospitalization for heart failure in adults with chronic kidney disease associated with type 2 diabetes.”

I use this medicine for all diabetic patients who have either kidney disease, high blood pressure, or protein in the urine (sometimes all three things exist together in the same patient).
Non-Diabetic kidney disease
Although we have neither any randomized-control trials to support the use of finerenone in non-diabetic kidney patients nor the FDA’s approval, there is enough observational data for such an application, and it is only a matter of months before Finerenone will get a green light for its use in non-diabetic patients.
I am using this medicine for all kinds of non-diabetic kidney disease, patients, say, for example, with Iga nephropathy and FSGS and membranous nephropathy, who have proteinuria despite a maximum dose of ARBs and SLGT-2 inhibitors. And with good results. Moreover, Finerenone’s blood pressure-lowering property makes it an attractive choice for blood pressure control in heart patients, whether they have kidney disease or not.
Anti-inflammatory and anti-fibrotic properties
What sets finerenone apart from other kidney-protective medicines is its anti-inflammatory and anti-fibrotic effects.
Inflammation from overactivation of the immune system underpins all non-diabetic glomerular diseases, resulting in kidney injury and proteinuria. To quell this inflammation nephrologists often use strong immune suppressive medicines. Finerenone, too, appears to have such anti-inflammatory powers, to a lesser extent, though. Just like corticosteroids, they alter the gene expression of immune cells, transforming pro-inflammatory cells into anti-inflammatory cells.

Finerenone brings about a similar change in the genetic expression of profibrotic cells, reducing the number and activity of fibrotic cells in the heart and kidney. Fewer fibrotic cells means less collagen, which means less fibrosis, which translates into a decreased risk of kidney disease progression and cardiovascular complications, plus a reduction in proteinuria. Fibrosis is a universal feature of all chronic kidney disease, and the anti-fibrotic potential of finerenone makes it a promising drug for not only diabetic kidney disease but kidney disease of any origin. This broader use of Finerenone just awaits validation from research.
Side Effects
The side effect profile of this new medicine is as charming as its list of benefits. There are only notable side effects. It can raise the potassium level in your blood, hence the warning by the FDA of not using this drug in patients with blood potassium levels above 5.
Another side effect is low blood pressure. Therefore, patients using Finerenone require their potassium and blood pressure to be regularly checked.
My personal experience
Initially, I reserved Finerenone for managing proteinuria alone, that too as a third drug, only after I had maximized the dose of the other two medicines—ACEIs/ARBs and SGLT-2 inhibitors. This soon changed. Now, Finerenone is my drug of choice for diabetic patients with protein in the urine. If a patient is not already on any of the traditional medicines and has a lot of proteinuria, I start Finerenone, dial it up to the maximum, and then add the other two drugs, all one by one.
I use Finerenone in non-diabetic patients, too, with no less success. In addition to its magic for proteinuria, this drug seems to be a godsend for high blood pressure.
Summary
Finerenone has a vast potential for kidney disease patients. Currently, it is FDA-approved for diabetic kidney disease patients only, but the observational data of minor trials and, more importantly, the clinical experience of physicians will soon propel scientists to scrutinize via randomized-control trials the benefits of this drug in non-kidney disease patients. Until then, we better serve our patients by using this medicine in as broad a kidney disease patient population as possible, as dictated, of course, by the clinical need.